1.2. Patient Assessment
General Examination and Anamnesis
In the assesment for fixed dentures, treatments that can be problem in the sense of physical or mental health of the patient and are non-obligatory should be postponed or canceled. In some cases, premedication may be required to prevent adverse health outcomes.
It should be questioned about Infectious diseases such as hepatitis or AIDS, and required precautions should be taken. There are also cases that are not contagious but important for the patient's health. If there is any possibility of an allergic reaction, it should be questioned and informed about the source of allergy by consulting the patient's doctor. Drugs or material that may cause any allergic reaction should not be used and their alternatives should be applied. Local anesthetics and antibiotics are among of such drugs. Measurement materials and nickel-containing alloys in particular are the substances which can cause such reactions.
Patients with cardiovascular disorders may need special treatment. Treatment should not be started without a normal level of blood pressure for such patients that are not under control. Generally, the treatment of the patients whose systolic pressure and the diastolic pressure exceeds 160 mm (mercury) and 95 mm (mercury) consecutively should be interrupted and it should be consulted with the physician of the patient.
Patients with a history of high blood pressure and cardiovascular disease should not be given drugs containing epinephrine. Epinephrine increases heart rate and blood pressure.
It may be required to be performed prophylaxis after consultation with patient's doctor for the patients who have heart valve implant, bacterial endocarditis, inherited heart diseases or rheumatic fever history.
Epilepsy is not an obstacle for dentistry, but an epileptic attack that the patient may have during treatment can make the required medical response difficult. Required precautions should be also taken to control the anxiety in these patients. Long, exhausting sessions should be avoided to prevent the epilepsy seizures.
If diabetic patients are under control, they can easily perform routine dental treatment. Uncontrolled patients, patients with high blood sugar and patients with a tendency to hyperglycemia can be badly affected with treatment stress and they can lapse into a sugar coma. Hypoglycemia can also cause problems. If diabetic patients who are under control do not eat regularly, they feel dizzy and look as if they got poisoned. Before starting treatment, it should be learned from patient's doctor whether patient can withstand dental treatment and sugar level is appropriately controlled.
The patient should be allowed to explain his complaint exactly. The dentist should make the necessary effort to clearly understand the patient's expectations after the treatment. Aesthetic expectations of the patient should be identified and it should be indicated the extent to which they can be met.
Oral Examination
In oral examination of the patient, oral hygiene is considered first. Dental plaque formation on teeth and general periodontal status are examined. Condition of the gums (inflammation and other signs), available periodontal pockets, location and depth of these pockets should also be determined. Such cases as tooth mobility and its amplitude, relationship between early touch in occlusion and whether the tooth can be used as a support should also be considered.
Toothless areas should be examined carefully. The relationships between the toothless areas, condition of the tooh/teeth which are intended to be used as support, tooth decays, previous restorations or unsuccessful treatments and reasons should be recorded.
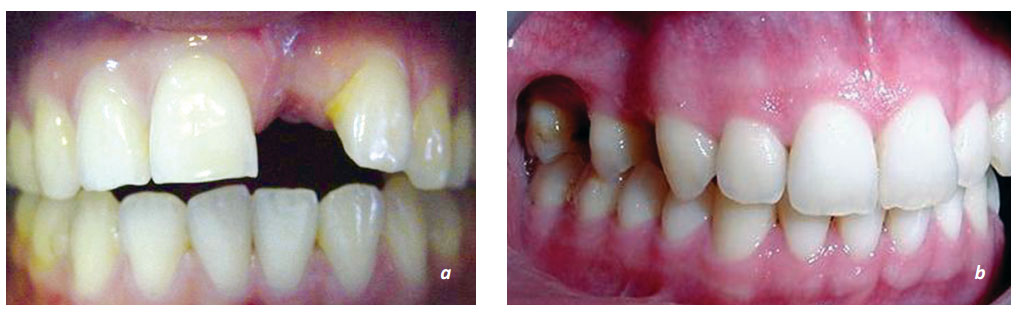
 Figure 1. 1 a,b,c. Tooth loss may occur one or more, adjacent or intermittently in the anterior or posterior region. The teeth in either side of the gap may be problematic, healthy or restorated.
Figure 1. 1 a,b,c. Tooth loss may occur one or more, adjacent or intermittently in the anterior or posterior region. The teeth in either side of the gap may be problematic, healthy or restorated.
Periapical, bite, occlusal or panoramic radiographs can be used as a support for the examination. Periapical radiographs give more detailed information. They should be carefully examined to determine the interdental decays and secondary decays occuring around the pre-made restorations.
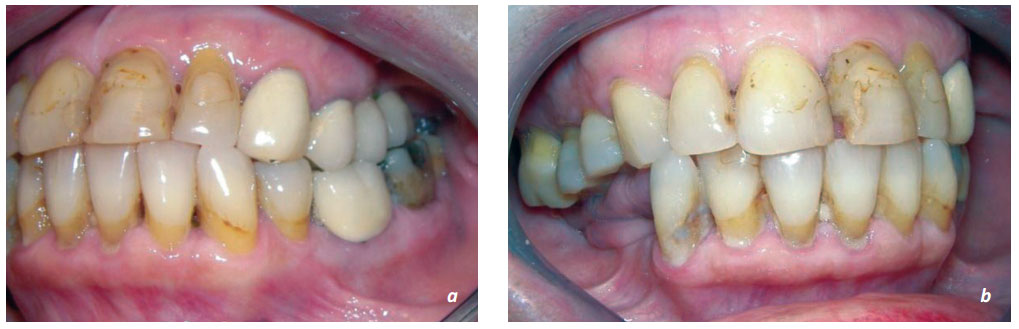
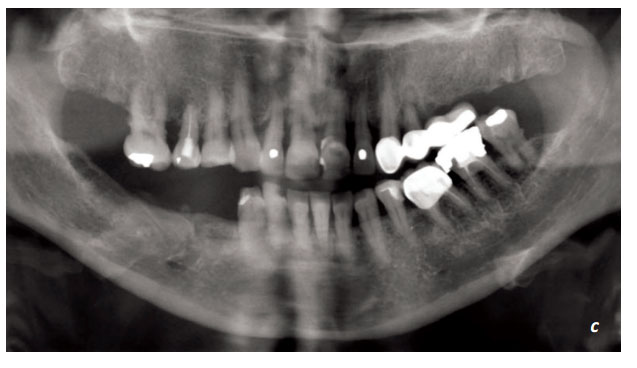 Figure 1.2. a, b, c. Pre-made restorations and their condition should be determined. It should be decided on their suitability and whether they will be changed or not. The radiographs support the clinical evaluation.
Figure 1.2. a, b, c. Pre-made restorations and their condition should be determined. It should be decided on their suitability and whether they will be changed or not. The radiographs support the clinical evaluation.

Figure 1. 3. a, b. The wear and tear of the teeth should be examined. The restorations should be performed for the wear caused by muscular diseases such as bruxism after the treatment is completed according to etiology. Effects on the restorations due to improper occlusal relationships of existing restorations, and wear of the natural opposing teeth shouldn't be overlooked.
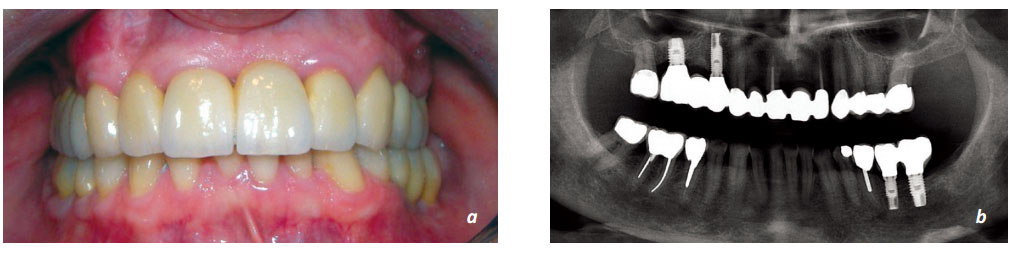
Figure1. 4. a, b. When the implants and prosthetic restorations applied 15 years ago were examined with panaromic radiograph, it is seen that there was no problem in all treatments and restorations.
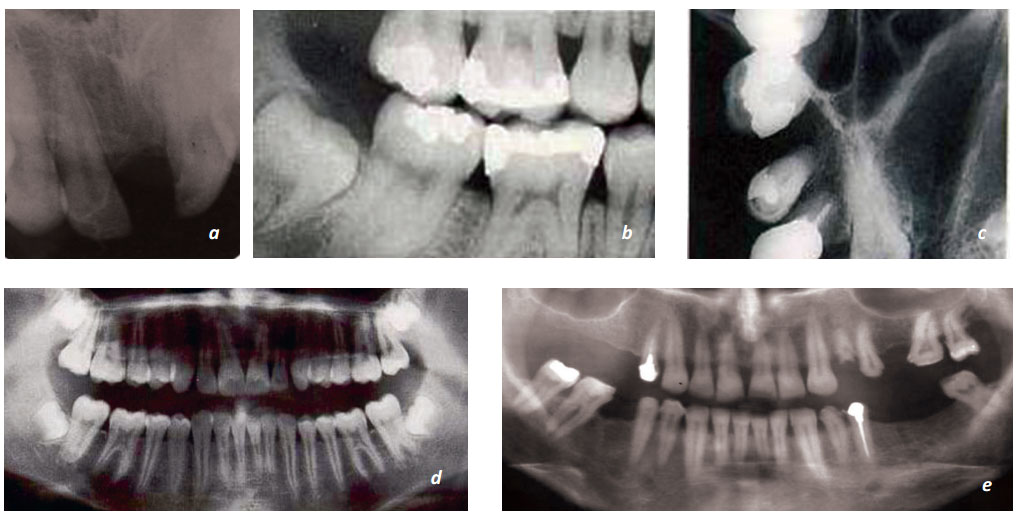
Figure 1. 5. Intraoral and extraoral radiographs are important during the examination. a. Periapical, b. bite, c. occlusal or d,e. panoramic radiographs can be used as a support for the examination.
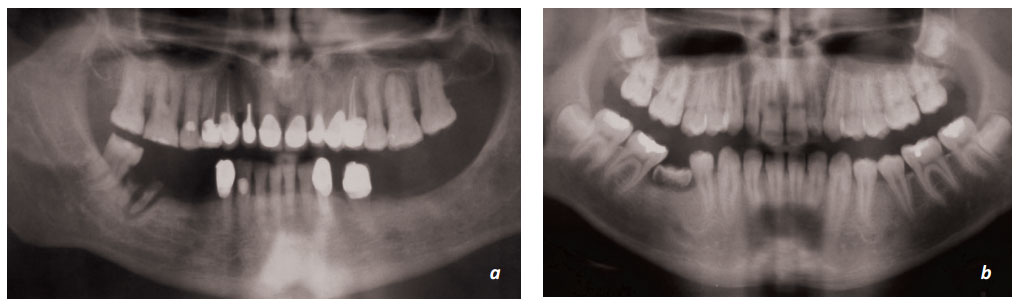
Figure 1. 6. a, b.The characteristics of periapical lesions and previous endodontic treatments can be determined by panoramic radiographs. The buried roots, teeth and other pathological elements in the toothless areas can also be determined.
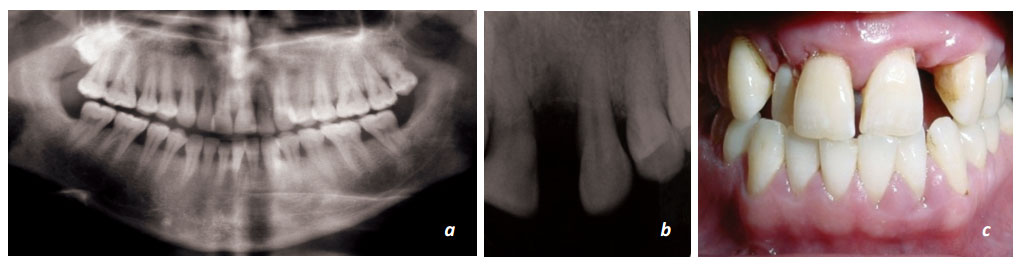
Figure 1. 7. a, b, c. At first, the gingival and alveolar bone levels (especially around of the support tooth/teeth) should be observed. The crown-root ratio of the support tooth should be calculated. The shape, length and direction of the roots should be examined. Any enlargement of the periodontium, the cortical bone layer around the tooth and bone trabeculae should be evaluated.
